















 231 320
231 320

Most studies reported stone sizes but did not report
stone location. Fewer than half of the studies contained
information on obesity (or body mass index). The risk of
confounding was moderate to high for previous open
surgery, access site, and access location, since only one or
two studies reported on these factors (
Fig. 2 ). The tract size
used and the stone types and locations (when reported)
were heterogeneous.
3.7.
Discussion
3.7.1.
Principal findings
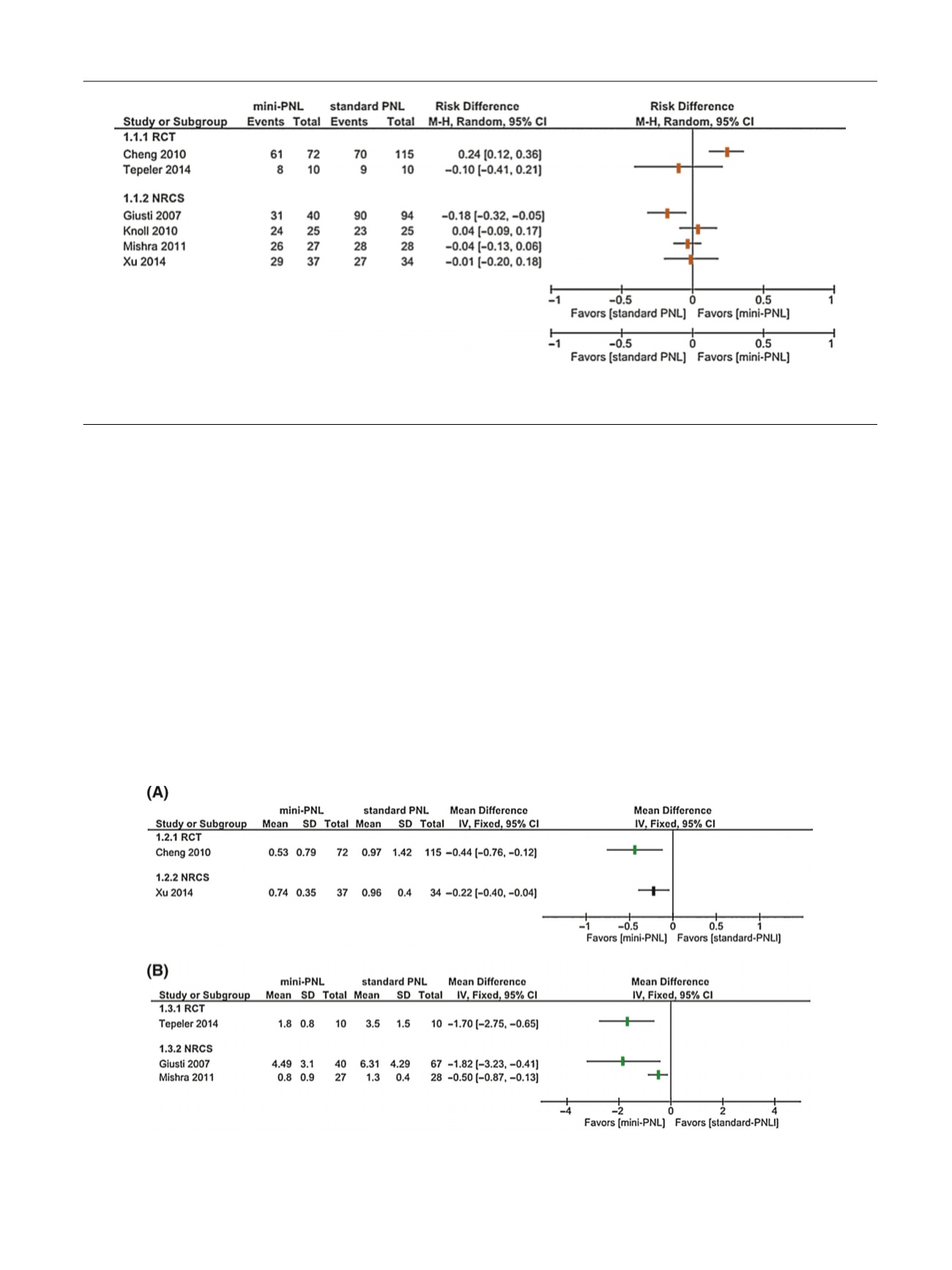
SFRs were comparable in patients with renal stones treated
with mPNL and standard PNL
( Fig. 3). Smaller tracts tended
to be associated with significantly lower blood loss (
Fig. 4 )or need for blood transfusion
[11,19,21,24,26–28]at the
cost of a significantly longer procedure
[11,19,24,28] ( Fig. 5 ). Hospital stay length was mostly shorter for mPNL
[11,22,24,34] ( Fig. 6). The studies were heterogeneous with
respect to tract and stone sizes, and the RoB and
confounding risk were generally high.
The terms used to describe tract sizes, such as ‘‘mini-
PNL’’, ‘‘ultra-mini-PNL’’, and ‘‘micro-PNL’’, have not been
well defined and partly overlap. In general, tracts sized 18
Fr are used for miniaturized techniques
[28,35]. Urologists
need to be aware that such terms describe not only the size
of the access sheath but also of specific instruments,
dilators, and operative concepts
[36–40] .This systematic
review indicates that mPNL is a safe and effective evolution
of the PNL technique, and thus warrants further investiga-
tion. RCTs are necessary to better assess the benefits and
harms in relation to both disease-related parameters (stone
size, quantity and location) and interventional parameters
(tract size, puncture locations, and intrapelvic pressure).
[(Fig._4)TD$FIG]
Fig. 4 – Forest plot showing the postoperative hemoglobin decrease in (A) g/dl and (B) percent reported in randomized controlled trials (RCTs) and
nonrandomized comparative studies (NRCSs). Reference numbers for studies are given in
Table 1 .PCNL = percutaneous nephrolithotomy; SD = standard
deviation; CI = confidence interval; IV = inverse variance.
[(Fig._3)TD$FIG]
Fig. 3 – Forest plot showing the stone-free rates reported in the randomized controlled trial (RCTs) and nonrandomized comparative studies (NRCSs).
Reference numbers for studies are given in
Table 1 .PCNL = percutaneous nephrolithotomy; M-H = Mantel-Haenszel; CI = confidence interval.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 2 2 0 – 2 3 5
231