















 270 320
270 320

performed with a 5-0 Gore-Tex (W. L. Gore & Associates,
Newark, DE, USA) suture with a single-layer running stitch
( Fig. 3h). Tourniquets are released sequentially (left renal
vein, suprarenal IVC, infrarenal IVC) and caval flow restored
( Fig. 3 i). Right RN and ipsilateral RPLND are then completed
in the standard fashion.
2.3.5.
Left-sided caval thrombectomy
The following maneuvers are different for left-sided tumors.
Temporary cessation of blood flow to the right kidney is
necessary to properly exclude the caval segment for
controlled thrombectomy. The right renal artery and vein
are controlled with individual bulldog clamps, prior to
cinching the infra- and suprarenal IVC tourniquets
( Fig. 4 a). The thrombus-bearing left renal vein is transected
with an Endo GIA stapler (left-sided tumors routinely
undergo preoperative angioinfarction)
( Fig. 4b and 4c).
After caval thrombectomy and reconstruction, caval flow is
restored and the right kidney revascularized. The patient is
repositioned left side up for left RN
( Fig. 4d) and ipsilateral
RPLND.
2.4.
Postoperative care and follow-up
Routine postoperative care, deep vein thrombosis prophy-
laxis, and early ambulation are performed. Postoperatively,
subcutaneous heparin is prescribed at a dose of 5000 U
every 8 hours. Upon discharge, prophylactic anticoagula-
tion with 40 mg enoxaparin sodium daily is continued for 1
[3_TD$DIFF]
mo. Follow-up includes a routine postoperative clinic visit
within 1–2 weeks of discharge that includes wound care
check, vital sign assessment, complication and functional
assessment, and medical oncology consultation as indicat-
ed. Follow-up then continues at 1 month, 3 months, and
then annually. Cross-sectional imaging, chest x-ray, and
laboratory investigations are done at 3 and 6
[4_TD$DIFF]
months and
per surgeon discretion thereafter.
2.5.
Data collection and statistical methods
Data were prospectively accrued in our renal database
approved by a institutional review board. Demographic
data included age, gender, body mass index, and American
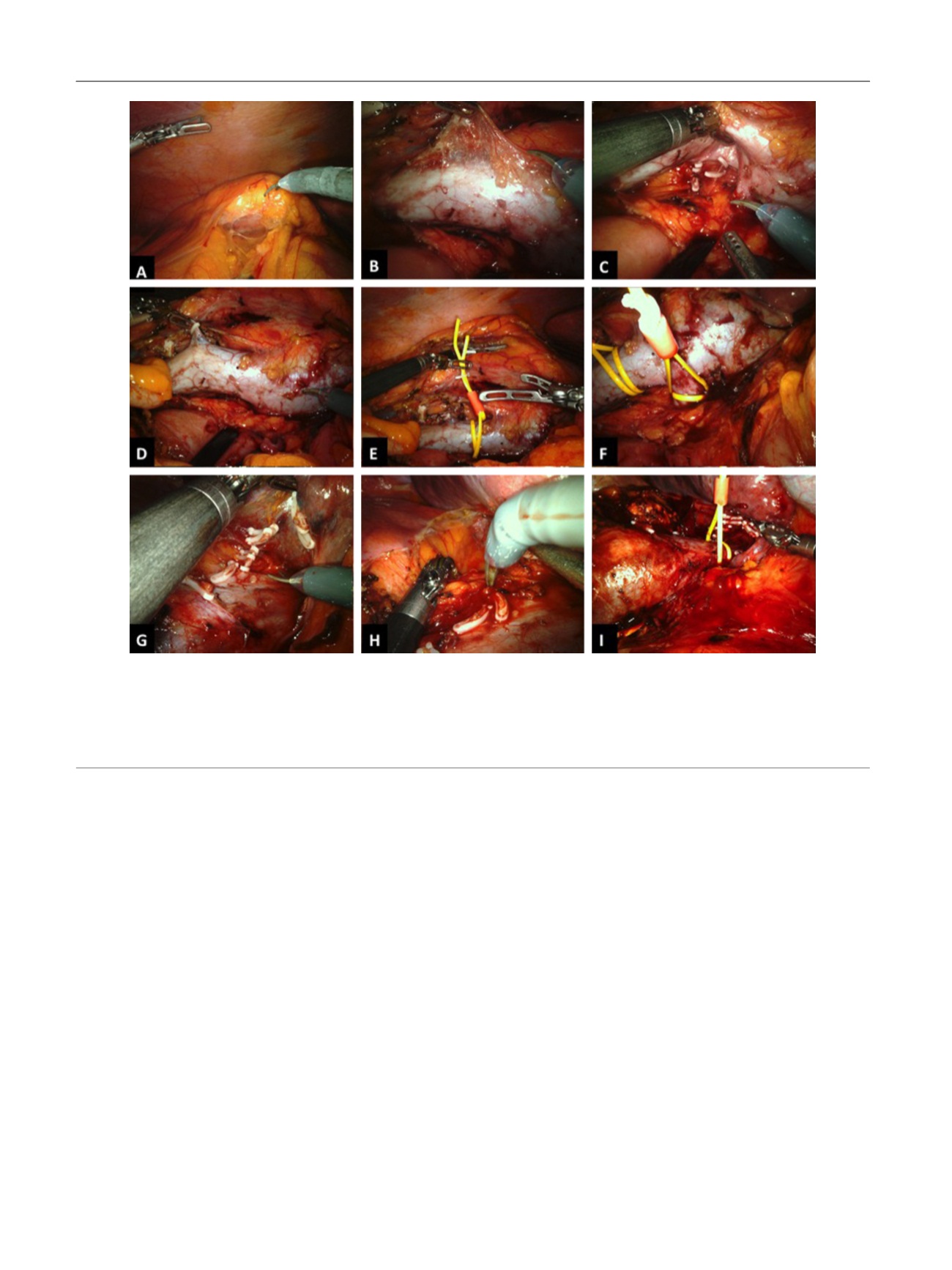
[(Fig._2)TD$FIG]
Fig. 2 – Vena caval control. (a) Dissection occurs to expose the vena cava; (b) the interaortocaval region is exposed; (c) the infrarenal inferior vena cava
(IVC) is dissected and lumbar veins are controlled; (d) the gonadal vein is controlled; (e) the infrarenal IVC is encircled with a double-loop tourniquet
(Rummel) using a vessel loop; (f) the left renal vein is encircled with a double-loop tourniquet (Rummel) using a vessel loop; (g) the suprarenal IVC is
dissected intrahepatically and short hepatic veins are controlled with Hem-o-lok clips; (h) the right adrenal vein is controlled with Hem-o-lok clips; (i)
the IVC proximal to the thrombus and in the high intrahepatic location is encircled with a double-loop tourniquet (Rummel) using a vessel loop. All
tourniquets are secured in place with a Hem-o-lok clip.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 2 6 7 – 2 7 4
270