















 239 320
239 320

1.
Introduction
The incidence of prostate cancer (PCa) has increased over the
past 2 decades due to the widespread use of prostate specific
antigen (PSA) screening
[1] .This trend is mostly marked in
low-risk localized PCa
[2] ,while a considerable reduction of
metastatic PCa at diagnosis has been reported
[3–5].
A significant challenge is to differentiate PCa destined to
cause clinical symptoms or metastases frommore clinically
indolent PCa that is highly unlikely to impact survival, even
without immediate treatment. To this aim, several risk
classifications have been proposed on the basis of clinical
and pathological characteristics such as clinical stage, PSA,
and biopsy Gleason score. Several local active treatments
have been proposed in this setting, such as radical
prostatectomy (RP), external beam radiotherapy (EBRT),
or active surveillance (AS). Although several different AS
protocols have been proposed, it generally consists of
monitoring with PSA, prostate exam, with or without
magnetic resonance imaging (MRI), and repeat prostate
biopsies. It differs from watchful waiting, which is a passive
approach where symptomatic progression prompts the
subsequent use of palliative treatment.
The aim of this review is to evaluate currently available
literature about low-risk PCa and to provide a contempo-
rary overview of diagnostic approaches and available
management options.
2.
Evidence acquisition
A literature review was performed in June 2016 using the
Medline, Embase, and Web of Science databases. The search
strategy included the terms ‘‘prostate cancer,’’ ‘‘low risk,’’
‘‘active surveillance,’’ ‘‘focal therapy,’’ ‘‘radical prostatec-
tomy,’’ ‘‘watchful waiting,’’ ‘‘biomarker,’’ ‘‘magnetic reso-
nance imaging,’’ alone or in combination. The search was
limited to English literature. References cited in selected
articles and in review articles retrieved in our search were
also used to identify manuscripts that were not included in
the initial search. The articles that provided the highest level
of evidence were then evaluated. When existing, prospective
studies were preferred to retrospective designs. A list of
articles judged to be highly relevant by the first and senior
authors was circulated among the coauthors and a final
consensus was reached on the structure of the review and the
articles included. The systematic review was performed in
agreement with the Preferred Reporting Items for Systematic
Reviews and Meta-analyses guidelines
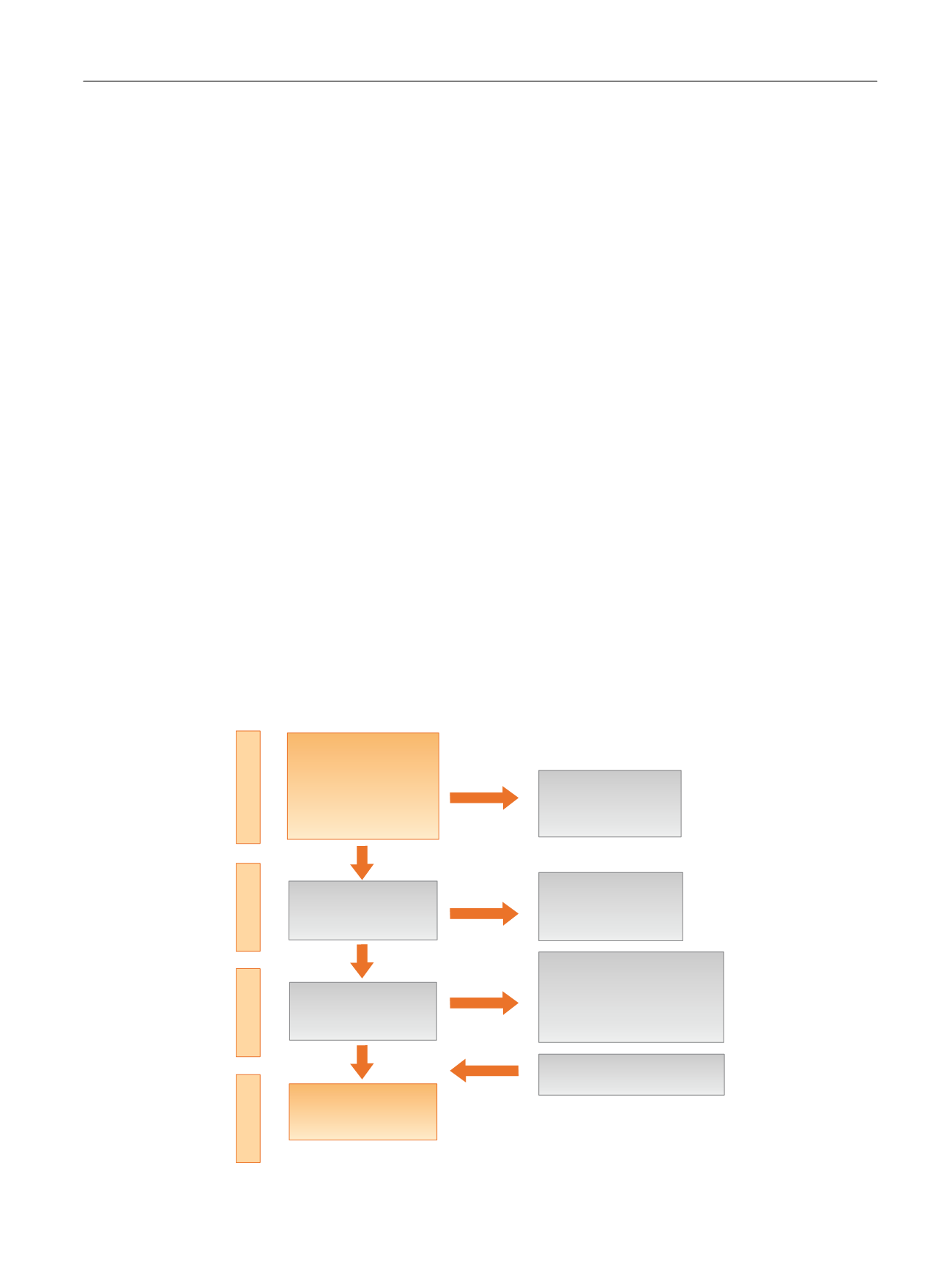
( Fig. 1)
[6] .3.
Evidence synthesis
Fig. 1shows a flow diagram of the selection process for this
systematic review of the literature. Out a total of 723 articles
screened, 189 were initially assessed for eligibility. Of these
121 were subsequently excluded and
[16_TD$DIFF]
31 were selected and
included by authors. In total,
[17_TD$DIFF]
99 articles were selected and
critically analyzed.
3.1.
Definition of low-risk PCa
Low-risk localized disease has generally been defined as
clinical stage T1–T2, biopsy Gleason score 6, and PSA
<
10
ng/ml. Almost all risk classifications utilize these risk factors
based on outcome data after whole-gland treatments
[(Fig._1)TD$FIG]
Unique records
identified from
search of medline,
embase, and web of
science databases
(
n
= 9435)
Nonrelevant records
excluded based on
title and abstract
(
n
= 8712)
Nonrelevant records
excluded based on
full text evaluation
(
n
= 534)
Excluded (
n
= 121):
Nonrelevant to this review,
same/overlapping series or
reviews/editorials
/commentary
Selected references
included by authors (
n
= 26)
Studies included in
qualitative
synthesis (
n
= 94)
Records assessed
for eligibility
(
n
= 189)
Records screened
for full-text
evaluation (
n
= 723)
Identification
Screening
Eligibility
Included
Fig. 1 – Flow diagram of evidence acquisition in a systematic review for patients affected by low risk prostate cancer.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 2 3 8 – 2 4 9
239